

By Peder Horner, MD – Originally posted on LinkedIn on July 26, 2018
Over the last few decades, there have been tremendous advances in new, minimally invasive, treatment options for men suffering from an enlarged prostate, also known as benign prostatic hypertrophy (BPH). This is a non-cancerous enlargement of the prostate gland that is very common in men as we age.
Common symptoms of BPH include: frequent urination (including multiple times during the night that interfere with good sleep hygiene), weak stream or inability to urinate, difficulty beginning urination, loss of bladder control, and can be a cause of hematuria (blood in urine). BPH is the most common cause of Lower Urinary Tract Symptoms (LUTS). If left untreated, the obstruction caused by BPH can result in frequent UTIs, bladder stones, bladder dysfunction, and even kidney failure in advanced cases.
How common is it? Very. While the condition usually starts after 40, 50% of men over 50 are affected to some degree. Once a man is over 80, it’s basically guaranteed that the patient will have some degree of BPH (90%), so it’s nearly ubiquitous if a man lives long enough.
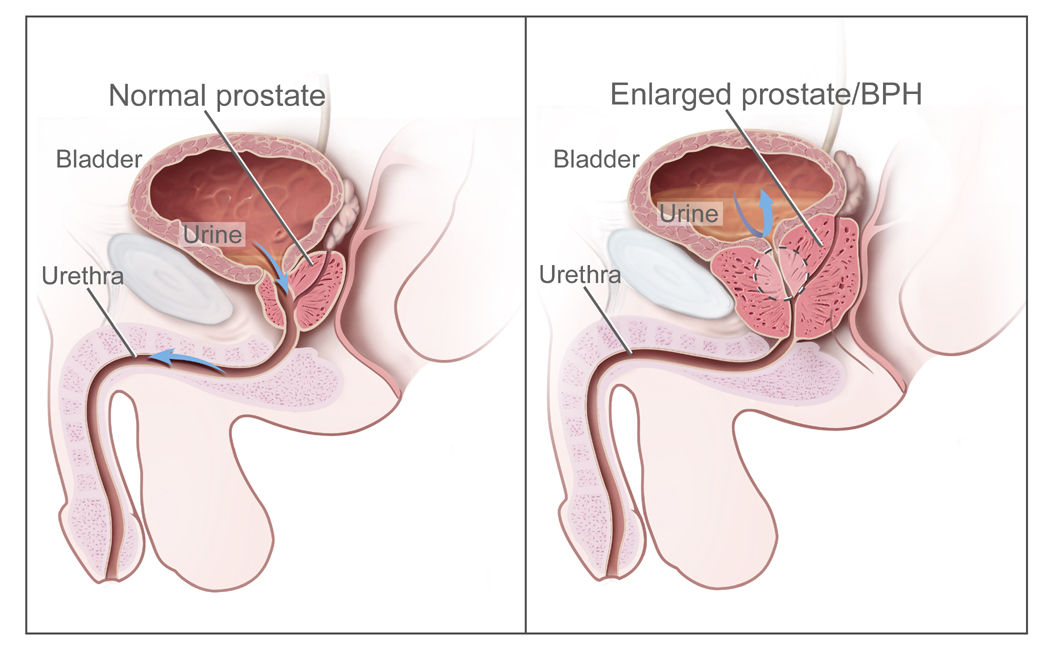
What causes BPH? No one really has a good answer for this. Some risk factors include diabetes, obesity, and lack of exercise. Family history does play a role in some cases. As the prostate gland enlarges, it presses on the urethra, which requires more bladder pressure to overcome, often leading to incomplete emptying of the bladder (and hence, the need to more frequently urinate).
How is it diagnosed? By physical examination and/or imaging studies (such as ultrasound, CT, or MRI).
What treatment options are available today? Lifestyle modification (reducing liquid intake before bedtime, avoiding/moderating alcohol and caffeine intake, and even voiding in the sitting position) and medications are the first line of treatment and can improve symptoms in most men. However, the medications do not fix the underlying problem, only help decrease the symptoms, and the treatment effect is incredibly variable from man to man. Side effects from the medications can also be bothersome.
Surgical – Many surgical procedures are available and offered by urologists. These include:
Open prostatectomy (good results, but considerably more invasive), TransUrethral Resection of the Prostate (TURP), Transurethral needle ablation (TUNA), Transurethral incision of the prostate (TUIP), Transurethral microwave therapy (TUMT), UroLift (implant), Rez?m water vapor therapy
Non-surgical – A novel approach to treating BPH in a minimally invasive fashion is Prostate Artery Embolization (PAE).
What is Prostate Artery Embolization (PAE)? PAE is a minimally-invasive image-guided (ultrasound and x-ray fluoroscopy) procedure provided by Vascular and Interventional Radiologists on an outpatient basis. The procedure is performed through the radial artery (wrist) or the femoral artery (tiny incision in the groin) under sedation. General anesthesia is typically not necessary. The procedure lasts around 1.5-2 hours and the patient is discharged from the hospital the same day to recover at home.
How does PAE work? PAE takes advantage of the fact that the prostate gland has a rich blood supply. By advancing a tiny (1 mm or less!) catheter through the arteries into the prostatic arteries, the blood flow to the prostate can be reduced by injecting small particles that lodge in the prostate. By reducing the blood flow to the prostate (embolization), the prostate responds by shrinking. This allows the urethra to return to a normal diameter, thereby increasing the urine flow rate, force of the stream, and more complete bladder emptying. These effects, in turn, result in far fewer trips to the bathroom, less urgency, and the ability to return to a more active lifestyle. Men can take control of their lives again, instead of worrying where the closest bathroom is at all times.
What are the side effects or potential complications? For a few days after the procedure, men who undergo PAE may uncommonly experience: “Post-PAE Syndrome” can last two to three days following the procedure and can include low-grade fever, pelvic pain, temporary painful or difficult urination, temporary urinary frequency, temporary small amounts of blood in urine and/or stool mixed with mucus, and blood in semen, potential skin burns from prolonged fluoroscopy (imaging), exposure to contrast dye can cause allergic reaction or kidney damage, rare embolization of non-target areas (i.e., bladder, rectum)
What are the advantages of PAE over TURP? Medical research into PAE has shown that PAE is a safe alternative to TURP with similar reduction in IPSS scores of 12-21 points and significant improvement in QoL scores. Unlike TURP, there is no risk of retrograde ejaculation with PAE. There is no known risk of Erectile Dysfunction or urinary incontinence with PAE either.
Is PAE for every man with BPH? There is no one-procedure-fits-all for men with BPH. Some men will be better treated surgically. But as experience and familiarity grow with PAE, I strongly believe more and more men will undergo the procedure. As a man who is getting older and may eventually have BPH myself, I certainly have a personal interest in keeping up with the latest and greatest treatments for enlarged prostate. When/if the time comes, I will certainly investigate all options with both an Interventional Radiologist and a Urologist.
Have questions about BPH and whether PAE might be right for you? Feel free to contact me through LinkedIn or email.
References:
Ask 4 PAE (patient information website)
Riad Salem, John Hairston, Elias Hohlastos, et al, Prostate Artery Embolization for Lower Urinary Tract Symptoms Secondary to Benign Prostatic Hyperplasia: Results from a Prospective FDA-Approved Investigational Device Exemption Study, Urology (2018), doi: 10.1016/j.urology.2018.07.012
McVary, KT, Roehrborn, CG, Avins, AL et al, Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803. PDF
Magistro, G, Chapple, CR, Elhilali, M et al, Emerging Minimally Invasive Treatment Options for Male Lower Urinary Tract Symptoms. Eur Urol. 2017. PDF
Cornu, JN, Ahyai, S, Bachmann, A et al, A Systematic Review and Meta-analysis of Functional Outcomes and Complications Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction: An Update. Eur Urol. 2015;67:1066–1096. PDF
Pisco, JM, Bilhim, T, Pinheiro, LC et al, Medium- and Long-Term Outcome of Prostate Artery Embolization for Patients with Benign Prostatic Hyperplasia: Results in 630 Patients. Journal of vascular and interventional radiology: JVIR. 2016;27:1115–1122. PDF
Kaplan, SA. Prostate Arterial Embolization is a Viable Option for Treating Symptoms of Benign Prostatic Hyperplasia: Con. J Urol. 2017;198:9–11. PDF
Carnevale, FC, da Motta-Leal-Filho, JM, Antunes, AA et al, Quality of life and clinical symptom improvement support prostatic artery embolization for patients with acute urinary retention caused by benign prostatic hyperplasia. Journal of vascular and interventional radiology: JVIR. 2013;24:535–542. PDF
Gao, YA, Huang, Y, Zhang, R et al, Benign prostatic hyperplasia: prostatic arterial embolization versus transurethral resection of the prostate–a prospective, randomized, and controlled clinical trial. Radiology. 2014;270:920–928. Pubmed
Aoun, F, Marcelis, Q, Roumeguere, T. Minimally invasive devices for treating lower urinary tract symptoms in benign prostate hyperplasia: technology update. Res Rep Urol. 2015;7:125–136. Pubmed
Bagla, S, Smirniotopoulos, J, Orlando, J et al, Cost Analysis of Prostate Artery Embolization (PAE) and Transurethral Resection of the Prostate (TURP) in the Treatment of Benign Prostatic Hyperplasia. Cardiovascular and interventional radiology. 2017;40:1694–1697. Pubmed
Learn more about other minimally invasive alternatives to surgery.